
National Standards:
- Crohn’s and Colitis UK

- IBD standards 2013 update:
- NICE – Feb 2015:
https://www.nice.org.uk/guidance/qs81/resources/inflammatory-bowel-disease-pdf-2098903535557
These are the 4 NICE standards:
- People with suspected IBD should be seen within 4 weeks.
- The services should be age-appropriate and supported by a multidisciplinary team.
- People having surgery for inflammatory bowel disease have it undertaken by
a colorectal surgeon who is a core member of the inflammatory bowel disease multidisciplinary
team. - People receiving drug treatment for inflammatory bowel disease are monitored for
adverse effects.
What is required to run a great service?
The commonly forgotten elements include – managerial, clerical support, Surgical, pharmacy, nutrition, pathology and psychological support. All of these and gastroenterology, IBD nurses, endoscopy access, radiology and much more are needed to set up a world-class service.
Where is the data?

Data is King! You need the data in order to get the money, and actually push forward your service.
We need to capture this to inform the patient, drive research, perform audit and benchmarking, plan the service and drive things forward at a national level.
At present we have:
- Hospital episode statistics
- NHS statistics
- IBD clinical teams
- Data from IBD patients
98 trusts are currently connected to the registry. 60 are connected to NHS digital.
This all feeds into NHS digital where it is pseudonymised. It is then passed to the IBD registry where it can be analyzed and deployed.
At present there are the following available platforms which patients can use:
- Patient view – this has come out of the renal patient view
- Patients Know Best
- IBD BioResource
- Improve Care Now – Paediatric IBD system
These above systems should hopefully help us to monitor the patients better in future.
Pharmacy:

The specialist pharmacist’s role is to monitor for changes in the liver function tests and other blood tests.
This will help to mitigate possible delays and cancellations.
They are heavily involved in the approval/funding process. NICE approval is subject to a 90 day implementation period. This is locally commissioned and agreed. After 90 days access is granted. Occasionally NHS England will commission the drugs to be given at specialist centers.
If people don’t meet the criteria then sometimes they require an individual funding request. Eventually, however, the ‘individuals’ become a group. At that time a group agreement is required.
Commissioning pharmacists are really important people when it comes to improving the service.
The pharmacy also keeps accurate records of who is on what biologic agent.
Drugs are classified as either:
- Blue – Primary care only,
- Green – Primary and Secondary.
- Yellow – specialist initiated/recommended but suitable for continuation in primary care (e.g mesalazine). In these situations there may be a shared care agreement in place.)
- Red – is for specialist use only (ie. Biologics).
Local shared care agreements are all listed in the West Hampshire CCG website. They exist for azathioprine, mercaptopurine, methotrexate, sulfasalazine, lubiprostone, and prucalopride.
Homecare is another part of an IBD pharmacists role. Home-delivered medications (such as Humira) attract a no VAT tariff so there is an incentive to do this.
Nutrition

The following criteria constitute malnutrition:
- BMI <18.5kg/m2 or
- Weight loss > 10% (indefinite of time) or > 5% in 3 months combined with either low BMI (age dependent) or low fat-free mass.
A lot of patients with IBD who are malnourished are actually BMI either normal or obese.
Nutritional deficiencies are common.
Micronutrient deficiencies are also common: magnesium and zinc, vitamin A&E, selenium and all the other common deficiencies are present in up to 30% of patients. (Vidarsdrottir et al.)
The dieticians spend some time discussing this all with the patients. A lot of patients have strictures and diet can help in preventing obstruction. Then addressing the malnutrition and maintaining the nutritional status, identifying food ‘triggers’, correcting deficiencies, reduce stomal losses (preventing dehydration), dietary treatment – liquid diets, and re-educating people about nutrition all form part of the IBD dieticians role.
Radiology
Roles of imaging
Diagnosis is for:
- Defining disease extent
- Assessing disease activity
- Extraluminal Manifestations
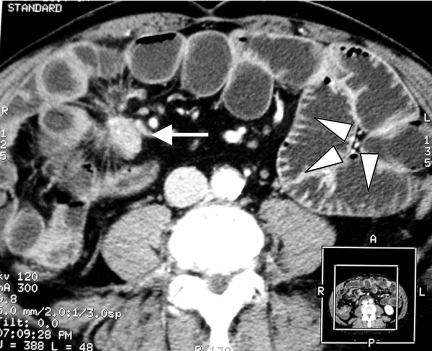
Often the first suggestion of IBD can be seen on CT scans.
Available Techniques with their respective pros and cons:
Fluoroscopy for the small bowel, enterography, and enteroclysis (enterography is oral and enteroclysis is via an NG tube). The barium bolus dives deep. Fistulograms and Loopograms are other options.
Fistulograms and Loopograms are other fluoroscopic techniques.
Pros: provides good luminal information at a relatively low dose.
Cons: No transmural or extraluminal assessment. The methylcellulose makes the patients feel sick. Plus, availability is limited.
CT – With or without IV or Oral contrast.
Can be enterography or often enteroclysis as well.
Pros: High spatial resolution and extra information, sensitive and reproducible.
Cons: Radiation, IBD patients are young. Not dynamic, lower contrast resolution (particularly without contrast).
MRI – Again can be with or without IV or Oral contrast.
Tends to be enterography.
Pros: Excellent contrast resolution. Different sequences, better neural detail. Reproducible. Dynamic.
Cons: Time consuming, access. (There are 5 or 6 at Southampton, but even despite this each study takes at least 30 minutes). Oral contrast is poorly tolerated. Reduced spatial resolution.
USS
Pros: No radiation. V.high spacial resolution. Doesn’t rely on dilatation.
Cons: Operator dependent, Less reproducible, Patient dependent (obese, scarred abdomens are difficult to scan.) The propensity for missing complications – abscesses and perforations.
Ustekinumab

A new biologic which has recently entered the IBD scene.
Most of the trials in IBD are now endoscopy based. Endoscopy + CDAI or Mayo score will be used to assess response.
If they respond then they stay on this arm of the study. If they don’t they either switch arm they go onto the open-labeled maintenance part of the study.
Lots of patients are excluded from trials because of comorbidities, a long disease duration, difficulties in treating them and fallibilities in the clinical scoring systems.
Ustekinumab is an antibody to IL-12 and IL-23. 3 trials: UNITI 1 and 2 + IM-UNITI.
UNITI 1 was for those who had failed on anti-TNF therapy.
UNITI 2 was for those who were TNF naive.
CRP’s and calprotectin’s are also improved.
Relapse studies were also done showing that those no placebo over a year are at a significantly higher risk of relapse.
The drug loading dosing should be weight based. It is administered in a similar fashion to adalimumab but there is a loading dose. Standard dosing is 12 weekly.
There are a lot of known potential side effects, as such, it is not advised as first-line biologic therapy. It is licensed for Crohn’s but not UC at present.
IBD in Pregnancy
The aim is for a:
1) Healthy Mother:
- Pre-Conception education,
- Control of IBD:
- drugs,
- Effect of IBD on pregnancy,
- Effect of pregnancy on IBD,
- Mode of delivery (think about long-term continence in some patients).
2) Healthy Baby:
- Drug exposure,
- Mode of delivery,
- The effect of IBD on the baby.
This area causes significant anxiety.
Many patients consider voluntary childlessness, half worry that they might not be fertile, two-thirds worry about passing the disease on to their children. This is not often discussed in clinic.
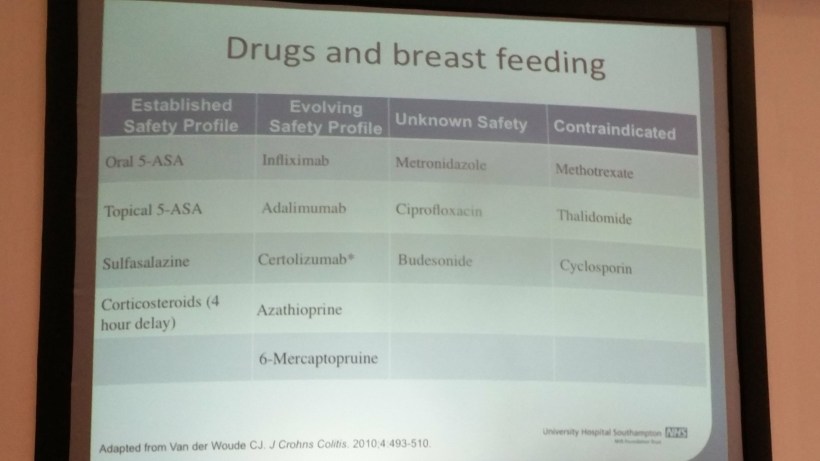
Regarding the drugs used in pregnancy: See the ECCO guidelines summarised below:

Ideally, patients should be in remission 3-6 months before they conceive. The chances of having a stable pregnancy are then much higher. The converse is also true so getting patients into remission early before conception is of paramount importance.
Treating depression can help IBD patients get pregnant!
The babies will arrive slightly earlier and be slightly smaller. There is an increased risk of severe perianal Crohn’s disease in some patients and some should be referred for a c-section.
Anti-TNF should potentially be stopped in the third trimester. This needs to be an individual decision.
Note: No live vaccines must be given for six months post delivery. (BCG, rotavirus, polio) – regardless of what you do during the pregnancy.
Post delivery certain drugs are also contraindicated during breastfeeding:
Getting the Diagnosis Correct – Excluding Infection

Rare infectious mimics –
- GI Schistosomiasis. Extremely difficult to diagnose, sometimes you can pick up the eggs on a colonic biopsy. Serology after about 3 months is highly reliable. Treatment is with praziquantel.
- HIV/Immunosuppression with other infections such as CMV, TB. Diagnosis of CMV is on PCR positivity on biopsy and viral inclusion bodies. The prognosis from CMV is poor.
- Other viral infections including VZV and HSV can also complicate the use of biologics and the consequences can be extremely serious. Infliximab is probably more immunosuppressing than adalimumab, which is more than others like etanercept. Particularly intracellular organisms in the first 90 days of administration. In particular septic arthritis (staph), TB, NTM, listeria, and Legionella are all associated. As are hep B, C, CMV colitis, HSV, VZV and respiratory infections. Apart from being screened for these conditions, the patients should have pneumococcal, influenza, and possibly hep B and VZV vaccination.
- Acute colitis can be mimicked by c.difficile and all sorts of other bacterial infections as well as some of the above viral causes and rotavirus. Near patient testing for gastrointestinal infections are currently under research.

You must be logged in to post a comment.