Proximie – augmented reality platform that allows surgeons/clinicians to collaborate in a AR platform.
Secure system – cloud based telesurgery. Allows you to work together locally and internationally. Crowdsourcing knowledge. Hardware agnostic. Virtually hands-on. Surgeons can reach the poorest from the richest areas.
AR is growing massively. What do the surgeons actually need? What does a consultant at home actually need?
They have now got some really diverse partnerships and have won some great awards.
She co-founded with a technical person and when they realised they were on to something they brought in a chairman and a director to make the team start to scale. It’s only when you have the idea, traction and team (with the right vision) that you can start to scale the business. They are now 25 strong! Good job!
Disclaimer: This article is meant for informational purposes only and not as clinical advice.
Warning: This article contains a few medical pictures
PSA / Prostate Cancer
First discovered in the 1970’s. Produced in the prostatic ductal epithelial cells it is normally involved in the liquification of semen.
Prostate Cancer risk rises with age. As dose PSA. However, the thresholds for investigation are becoming lower and lower. Even a 30 year old, a PSA over 1 would warrant further investigation. Family history, recent instrumentation, racial origin, other genetic factors and drug/past medical history also all need to be taken into account.
PR exam, heavy cycling, BPH, urinary retention, prostatitis and UTI’s can all falsely elevate the PSA.
Older patients are less likely to have major surgery (prostatectomy etc). There is a 1% risk of sepsis following a prostate biopsy as well so this procedure has to be done with due consideration for the risks. There are newer tests such as MRI prostate and ‘template’ biopsies which are helping to get higher yields.
Anyone who has visible haematuria (blood in the urine) without an obvious cause needs to investigated. If the haematuria is invisible then there need to be two separate positive urine dips. In the major paper on this – Edwards et al, 2000. of almost 2,000 patients with visible haematuria 24% were found to have a urological malignancy.
haematuria by dilution
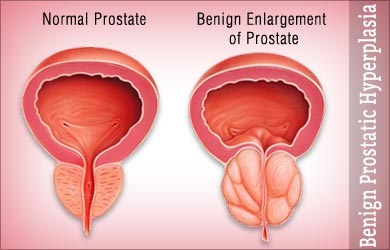
BPH
BPH (Benign Prostatic Hypertrophy) is a histological diagnosis. The cause is not exactly known but it is to to do with adenomatous change in the prostate which pushes on and obstructs the ureter.
They will tend to have impaired flows and high post-void residual volumes on bladder scan. This doesn’t predict the likelihood of people going into retention but it does predict risk of needing treatment. If the post-void residual is >150mls then urologists recommend avoiding ‘anticholinergic’ medications.
Various treatment options for BPH include: alpha-blockers (these work over about 24 hours), 5ARIs – (dutasteride), anticholinergics, transurethral needle ablation, microwave thermotherapy.
Catheters
Some patients cannot be catheterised. If two tubes of instillagel fail try a Tiemann Tip catheter. In an emergency the bladder can be aspirated using a green needle transabdominally. Urologists however should be involved at this point. Irrigation stops future clots being formed. Washouts are needed to get rid of the clots. If this doesn’t work then they will need to go to theatre.




You must be logged in to post a comment.