Healthcare services, Digital Health, Social Care, Medical products & Services are the four sectors they invest in.
They invest in high quality startups with scalability and the ability to save the healthcare service.
I then asked a question about how to penetrate the system and bring in change.
They feel that in the area of digital health there is going to be another healthcare economy outside the traditional one. The speed on progress and innovation is so great that the old system cannot keep up.
He feels any negotiations with the health service should start with healthcare economics.
By proving that costs will be cut either by efficiency savings or reduction of demand you can engage cash-strapped health services.
Apposite capital’s lifteime investments tend to be in larger companies who are already disrupting in health.
The best place to get seed capital is from rich friends/relatives. Then angel investors. If you choose the right angel you will do well. However, if you get a ‘bad’ angel they won’t be able to help you so much. Then next would be family offices. Grants and VCT’s – they see so many ideas they can help you refine your idea and decide whether or not it is worth pursuing.
The key for VC’s is growth. If you get a business up and running in a high growth sector a VC firm will be interested because even if the investment just keeps up there will ultimately be a good return on the investment. That is the biggest key for a VC firm and it is why the investments they make are so large.
A venture capital firm: Forward partners. Based in London explained what they could offer.
They are a VC firm who back very early-stage investments.
He discussed angel investing and other options,
Crowdfunding – 2-4 times what a VC
Banks
Accelerators – he doesn’t think these are so important
Grant money (get the free money first!)
Optimise your crowdfunding process. You need to think strategically. Getting the money is nor as important as getting it from the right source. List all your options and do your homework to make yourself ready. He talked about what investors are looking for.
Then he talked about why they are so excited about healthtechnology. It is a massive market (containing biotech and healthtech), eventually the two will fuse.
Trends they are interested in:
Mobile trends – people are constantly interacting with them and they are only going to grow as key connectors to customers.
IoT and Sensors – watches and beacons.
AI & Machine Learning – these analyse the data created by the sensors.
He gave the example of Amada in the US and their work with diabetes.
Basically there is big money available for those who have the skill and imagination to build results.
There is a fear that there is a lack of leadership within the NHS.
There is also a major difference between the current leading generation and those coming. The current generation is very traditional. In general the current leading generation will stick to what worked before and just keep going. The coming generation want instant feedback, (my generation stands in the gap but I lean toward the millenial side).
This new generation poses a significant threat to the new generation and can make it difficult to relate. If the design of the workforce has been performed by the older generation it will be the younger generation which will have to live with it.
You can either be an ostrich, king Cnut or a surfer. Click the pictures to see what they each do?
Ostriches hide from the sea
King Cnut tried to stop it
Surfers observe it and try to catch the wave
There are all sorts of regulatory bodies including NHS England, CQC, CCG’s, Dept for Health, HEE, NHSi and all sorts of other groups within the NHS. They each have different focuses and each try to get things ready for the future.
They are all working to this 5 year forward view plan. This involves commissioning of services (a mechanism involving competing for contracts and payment for services ‘commissioned’, networks are being built to try and connect different services (ie. Diabetes) to try and save money. Often the money is given in ‘packets’ which have to be spent quickly. You can build business cases which are ready to go at the drop of a hat to try and access this money.
Then there are clinical senates. These are groups led by clinicians to provide multidisciplinary input to strategic clinical decision-making. The groups, 12 of which are due to be established, should help to provide clinical input to the other decision making bodies.
A new relationship with patients and communities, Getting serious about prevention, Empowering patients, Engaging communities, The NHS as a social movement
Chapter Three – What will the future look like?
New models of care – Emerging models, One size fits all? New care models, How we will support local co-design and implementation
Chapter Four – How can we get there?
We will back diverse solutions and local leadership, We will create aligned national NHS leadership, We will support a modern workforce, We will exploit the information revolution, We will accelerate useful health innovation, We will drive efficiency and productive investment.
Prevention is much more important than cure. This has to become top priority if we are to change the NHS structure and culture and ultimately reduce costs.
Motivational interviewing, telehealth (Airedale model worked), urgent and emergency care networks, enhanced care in care homes. Multispecialty community providers, primary and acute care systems.
Heavy investment in general practice. 5,000 extra GP’s and 3,000 extra mental health practitioners.
Then we discussed trappist monks (as below). August Turak’s book shows that the key factors needed for success are: clarity of mission, faith in the mission, service and selflessness, commitment to excellence and trust. Does your organisation have these factors?
Will the NHS have this clear why? This is what the FTP’s are about. Joining up care and having a common vision.
Speakers ending comment: Think creatively, learn to play the game and you can surf the waves and succeed to make healthcare better for patients.
I learned so much from this guy I had to share it with others…
Now is the Time
Why bother starting a lifestyle business. You are sitting on so much value and you want to share that with the world not just make your life easier. you don’t want a checklist business!
‘Big will not beat small anymore. The fast will beat the slow’ — Rupert Murdoch. Even he is aware of it.
Ask yourself: Where can your business be in 12 weeks?
Incumbents should note that there are hidden ‘gun’s’ (startups) in peoples garages which contain bullets with other companies names on them.
As an investor, John Spindler finds the lack of background research by entrepreneurs to be one of the most commonly encountered frustrating problems. To solve this he suggested:
Make 2 columns:
Fact column- 2–3 facts you KNOW about this business plan.
2. Second column- Hypotheses. What things do I need to find out to build this thing?
Work out what is your OPPORTUNITY HYPOTHESIS. Build, Measure, Learn. Call it a project rather than a business because it is easier to fail fast. (I like the psychology of this idea and have already found it helpful).
In the experimental stage check your are measuring the right metrics, evaluation of them will lead to excellent execution.
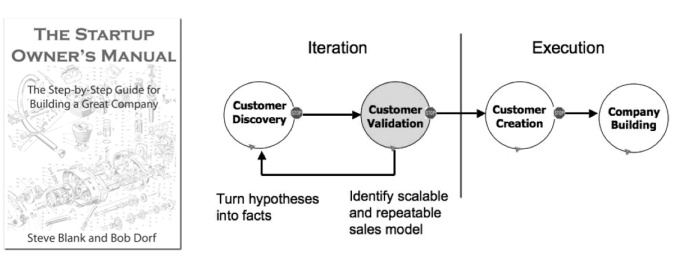
Startup Owners Manual: Steve Blank and Bob Dorf
Don’t build something nobody wants
3 types of advice: validated, negative and useless. (Validated/Negative advice in 8 weeks can be tested to see if it works. Good or bad it will help you. )
However, 95% of advice is useless in the next 8 weeks. Therefore, shelve it because it’s useless to you now.
Lean is just about organising the chaos, reducing waste and risk, providing more learning and a common language. IF your core assumption is wrong you need to test that FIRST. Then you will save yourself a lot of time.
It’s a common language. There is jargon and as soon as you learn it you can communicate with others — be ‘in the club’ as it were.
If you are going to build, do a lot of thinking. Then build the thing that teaches you what you need to learn.
The number one thing an investor will look at is the team. If you can convince a quality person to join you that is a sign of success. If you can recruit a quality army this is your number 1 asset! What quality of ARMY can you recruit? Investors will care about this more than anything else as it is the biggest single determinant of success.
Get OTHERS to validate your product. Your own validation is not that valuable but multiple external validations are.
Testing Hypotheses
A good hypothesis is simple & clear, written as a statement, establishes participants (who), variables (what’s involved) and prediction of an outcome (evidence).
The Pepsi Challenge type scenario is NOT the right first validation exercise. You have to assume that the first answer is wrong. Ask 5 why’s & eventually you might get to the nub of it. AVOID CONFIRMATION BIAS like the plague.
Most people are NOT early adopters in ANYTHING. Most people have habits that are very hard to break.
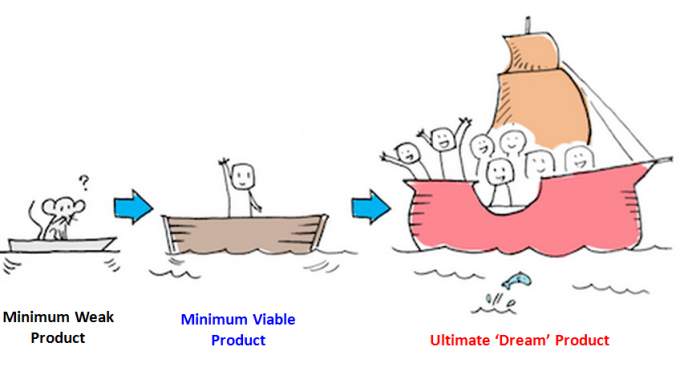
MVP is not a crappy version of the product. It is a prototype. Consierge MVP is legitimate. It can be a simple landing page, it can be a proof of concept, it can be something for people to engage with, it can be a paper prototype, a pitch, fake demo video, or something to help a developer to understand. It is just a way to answer the questions you need to answer.
Consierge means it is not scalable. It’s just there to allow you to learn. Beware, If your hypothesis is circular then its not a hypothesis and you need to think again.
Key assumptions you need to make
At least several other people are working on the same thing right now. How you think this your business idea will work is probably wrong. Your main job is to learn faster than the competitors. That is why the team is the key. It is the process and the people that win NOT the product itself.
The market is not stable and anyone who doesn’t keep moving forward will fall behind.
Call it a project, give it a name, sell something, convince someone else to join, set a goal that will inspire you, live 6 months in the future, fall in love with the problem and not your solution. Follow Peter Thiel’s philosophy as per ‘Zero to One’ (find it on Amazon its a good book.)
Teams
There are two types of teams. Napoleon team — they will follow your every command. The best teams however are people who are smarter than you and can do things you can’t and you bring them on the journey with you. They don’t want to just be footsoldiers for your army.
Bare minimum you need a hipster (domain insight), hacker (builder) and hustler (seller) to succeed.
Paul Graham- You need three things to be a successful entrepreneur — a great team, proof that customers want it and a willingness to do it with minimal money!
Regarding Customers
‘Make something people want’ — Paul Graham, Y Combinator
Avoid wasting too much time trying to change the ‘stuck’ middle who don’t want to innovate because they are very good at using the current system. Are your people your assets or your problem?
Before building your business ask: What problem would someone else solve for me?
Another thought: The number of secrets in the world is roughly equivalent to the number of startups we need.
How did the companies that are currently successful scale. When you scale big you win even if your product is inferior. Unless you can bring 10* value you are unlikely to be able to displace an incumbent. (As per Peter Thiel).
Design Thinking
He would thoroughly recommend doing Stanford’s online course on design thinking (8–10 hours). Emphasise, define, ideate, prototype, test. Do it in groups if you can, it will radically transform your thinking.
‘Kick Ass’ products have evidence that they solve a customers problem in a big market. Focus on the early adopters. People you can beta test with. Commit 5 people. They need to know they are aren’t buying a perfect solution.
They are trying to find a home made solution. They want you to succeed, they will give you their time and honest feedback and you have a relationship of trust. Your mum is not one of these first customers!
Do you know the demographic? Needs and goals? Problems that need solving, Present behaviours? How do they go about solving those problems? Reference group? The behaviours and the psychology are key.
Behaviour Change
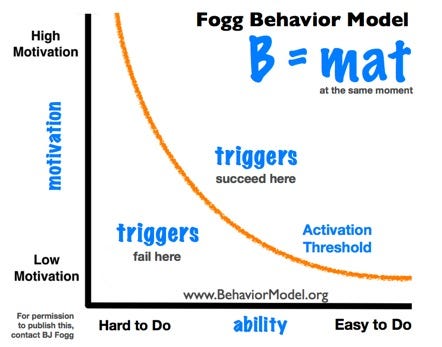
BJ Fogg. Head of behavioural theory at Stanford. B=mat. B=behaviours, m=motivation, a=pre-acquired ability, t=triggers (we are all contextual. We need external triggers to get us to change our behaviour. Every product is a behaviour change. Activation threshold affected by these three things, the triggers have to be enough to get them over the threshold.
Source: B.Fogg (Stanford) Site as per diagram.
Can you make something better than it already is? make something simpler? In an ideal world how would this problem be solved? Better, Simpler or emerging methods?
He suggests we build 5 actual profiles of 5 potential customers (actual people) . The more specific the better: Motivation, Habit , Income, Age, Location, Status, Backstory. Become intimately acquainted with there problems.
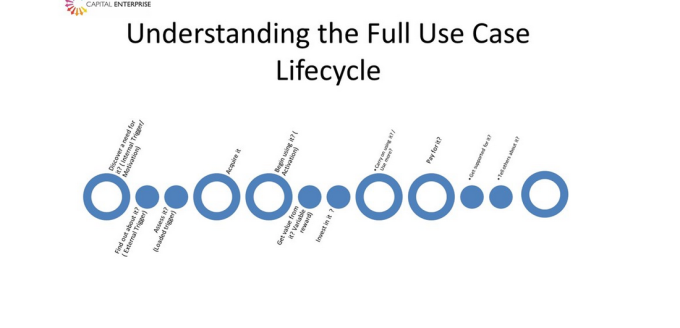
Then understand the full use-case lifecycle.
Source: @capenterprise — John Spindler
What do these personas do when ‘triggered?’
Entrepreneurship is a career. Startups are risky experiments. You don’t have to experiment full time. Start today with what you have.
Do you invest in startups who don’t use lean methodology? Yes but its rarer. Sometimes people just get damn lucky and hit a home run of first base but its the exception rather than the rule and it might not be repeatable.
Then he talked about financing and how ‘founders fit’ and how investors look at these things. Do you have someone resourceful, someone who can do x and y. The team you build now might well not be the team that takes it to the next level. Identify the task in hand and see if the team members can get you there.
Funders and investors must fit. An investor should never distort the function of the startup because this is your task. You have the hands on the controls. They are investing in you!
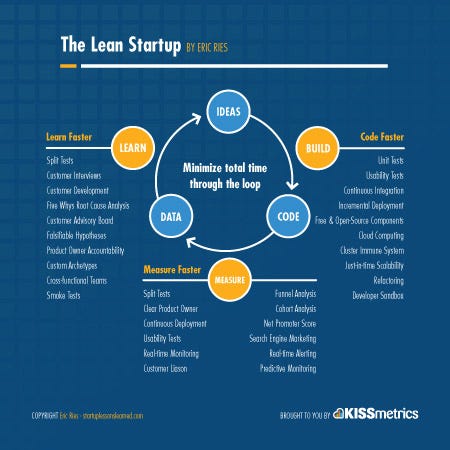
Suggested reading: Moms test by Rob Fitzpatrick, Running Lean by Ash Maurya and Lean Startup by Eric Ries.
This article came out of notes I took on a talk by @capenterprise at the first NHS clinical entrepreneurs pit stop – The beginning of a new journey. Or see my medium blog
Because the NHS is squeezed from all sides this provides a great escape valve for trusts if the innovation can be scaled and used across the board to improve efficiency. The AHSN’s and other groups have developed to help facilitate this and there are now various financial incentives appearing via NHS reimbursement schemes.
The Clinical entrepreneur programme has come about precisely because this need has been recognised. Late definitely beats never, and this in conjunction with the NHS accelerators will hopefully start to gain traction and lead to #development.
‘Make something people want’ – Paul Graham, Y Combinator
Avoid wasting too much time trying to change the ‘stuck’ middle who don’t want to innovate because they are very good at using the current system. Are your people your assets or your problem?
Before building your business ask: What problem would someone else solve for me?
Another thought: The number of secrets in the world is roughly equivalent to the number of startups we need.
How did the companies that are currently successful scale. When you scale big you win even if your product is inferior. Unless you can bring 10* value you are unlikely to be able to displace an incumbent. (As per Peter Thiel).
Design Thinking: He would thoroughly recommend we all do Stanford’s online course on design thinking (8-10 hours). Emphasise, define, ideate, prototype, test. Do it in groups if you can. Great course
‘Kick Ass’ products have evidence that they solve a customers problem in a big market. Focus on the early adopters. People you can beta test with. Commit 5 people. They need to know they are aren’t buying a perfect solution.
They are trying to find a home made solution. They want you to succeed, they will give you their time and honest feedback and you have a relationship of trust. Your mum is not one of these first customers!
Do you know the demographic? Needs and goals? Problems that need solving, Present behaviours? How do they go about solving those problems? Reference group? The behaviours and the psychology are key.
BJ Fogg. Head of behavioural theory at Stanford. B=mat. B=behaviours, m=motivation, a=pre-acquired ability, t=triggers (we are all contextual. We need external triggers to get us to change our behaviour. Every product is a behaviour change. Activation threshold affected by these three things, the triggers have to be enough to get them over the threshold.
Source: B.Fogg (Stanford) Site as per diagram.
Can you make something better than it already is, make something simpler. In an ideal world how would this problem be solved. Better, Simpler or emerging.
John suggests we build 5 actual profiles of people. The more specific the better. Motivation, Habit , Income, Age, Location, Status, Backstory.
Understand the full use-case lifecycle.
You need a hipster (domain insight), hacker (builder) and hustler (the first two work for him for free!).
Source: Capital Enterprise – John Spindler
What do these personas do when ‘triggered?’
Entrepreneurship is a career. Startups are risky experiments. You don’t have to experiment full time. Start today with what you have.
Suggested reading: Moms test by Rob Fitzpatrick, Running Lean by Ash Maurya and Lean Startup by Eric Ries.
Brilliant start to the clinical entrepreneur programme. @Tonyyoung and @theonlytoby introduce the programme (below)
Building a culture of entrepreneurial strength should be at the heart of what we are doing.
John Spindler @capenterprise – Lean Startup
Why bother starting a lifestyle business if you are a doctor. You have so much value and you want to share that with the world not just make your life easier. you don’t want a checklist business!
‘Big will not beat small anymore. The fast will beat the slow’ – Rupert Murdoch. Even he is aware of it.
Where can your business be in 12 weeks?
‘There are hidden gun’s in peoples garages which contain bullets with other companies names on them.’
As an investor, John Spindler finds the lack of background research by entrepreneurs to be one of the most commonly encountered frustrating problems.
2 columns:
Fact column- 2-3 facts you KNOW about what you about about do with this business.
Second column- Hypothesis. What things do I need to know to build this thing?
What is your OPPORTUNITY HYPOTHESIS. Build, Measure, Learn. Call it a project rather than a business because it is easier to fail fast. Like the psychology of this.
Experimental stage, metrics, evaluation leads to excellent execution.
Don’t build something nobody wants!
3 types of advice: validated and negative (in 8 weeks you can test it and see if it works. Good or bad it will help)
95% of advice is useless in the next 8 weeks. Shelve it because it’s useless.
Lean is just about organising the chaos, reducing waste and risk, providing more learning and a common language. IF your core assumption is wrong you need to test that FIRST. Then you will save yourself a lot of time.
It’s a common language. There is jargon and as soon as you learn it you can communicate with others – be ‘in the club’ as it were.
If you are going to build do a lot of thinking. Then build the thing that teaches you what you need to learn.
The number one thing an investor will look at is the team. If you can convince a quality person to join you that is a sign of successfulness. If you can recruit a quality army this is your number 1 asset! What quality of ARMY can you recruit? Investors will care about this more than anything else as it is the biggest determinant of success.
Get OTHERS to validate your product. Your own validation is not that valuable but multiple external validations are.
A good hypothesis is simple & clear, written as a statement, establishes participants (who), variables (what’s involved) and prediction of an outcome (evidence).
The Pepsi Challenge type scenario is NOT the right first validation exercise. You have to assume that the first answer is wrong. Ask 5 why’s eventually & you might get to the nub of it. AVOID CONFIRMATION BIAS like the plague.
Most people are NOT early adopters in ANYTHING. Most people have habits that are very hard to break.
MVP is not a crappy version of the product. It is a prototype. Consierge MVP is legitimate. It can be a simple landing page, it can be a proof of concept, it can be something for people to engage with, it can be a paper prototype, a pitch, fake demo video, or something to help a developer to understand. It is just a way to answer the questions you need to answer.
Consierge means it is not scalable. It’s just there to allow you to learn. If your hypothesis is circular then its not a hypothesis.
Key assumptions: At least several other people are working on the same thing right now. How you think this your business idea will work is probably wrong. Your main job is to learn faster than the competitors. That is why the team is the key. It is the process and the people that win NOT the product itself.
The market is not stable and anyone who doesn’t keep moving forward will fall behind.
Call it a project, give it a name, sell something, convince someone else to join, set a goal that will inspire you, live 6 months in the future, fall in love with the problem and not your solution. Follow Peter Thiel’s philosophy as per ‘Zero to One’ (find it on Amazon its a good book.)
Don’t call it a business because you will overprotect it. Call it a ‘project’. Get people to devote time to your thing.
There are two types of teams. Napoleon team – they will follow your every command. The best teams however are people who are smarter than you and can do things you can’t and you bring them on the journey with you. They don’t want to just be footsoldiers for your army.
Paul Graham- You need three things to be a successful entrepreneur – a great team, proof that customers want it and a willingness to do it with minimal money!
Then questions:
Do you invest in startups who don’t use lean methodology? Yes but its rarer. Sometimes people just get damn lucky and hit a home run of first base but its the exception rather than the rule and it might not be repeatable.
Then he talked about financing and how ‘founders fit’ and how investors look at these things. Do you have someone resourceful, someone who can do x and y. The team you build now might well not be the team that takes it to the next level. Identify the task in hand and see if the team members can get you there.
Funders and investors must fit. An investor should never distort the function of the startup because this is your task. You have the hands on the controls. They are investing in you!
I am a medical doctor who has been practicing for 6 years in the British NHS.
The NHS is a great institution. It has brought help to anyone at their point of need for over 68 years. Founded by Aneurin Bevan on 5th July 1948. Built as an instutition by the people, for the people it has certainly been (historically anyway) far from the insurance based systems of the US or the more industrial-type approaches of some other nations towards health. Quite rightly it is something that British people remain proud of.
Acutely Diseased?
However, it was founded at a time when acute illness was more common than chronic disease. It was also founded on a flawed assumption that if you made everyone better then the population as a whole would be healthy. This is unfortunately only true in part; as we are now painfully aware — if you make people better from their acute illness then eventually they live long enough to develop chronic diseases which are not so easily ‘cured’.
You see hospitals are not (and never were) really built for managing chronic diseases. As soon as you take away the specialist hospital input on discharge that person is still left with the problem but has to deal with it largely alone. At this point a hospital building is of limited use.
What, so doctors aren’t special anymore?
Essentially in a word, no. (There you go I have done it). Back when there was no alternative people just accepted it. However, a second key change happened in 1989 which sowed the seed which would eventually change that. When Tim Berners-Lee (disagree with me if you want to) came up with the world wide web the possibilties this would lead to were unknown. Still 27 years on they are largely unrealised, but in 1998 Google made the web searchable (again feel free to disagree); only now are we starting to feel the full effects of this seizmic change.
What this primarily means is that information is now cheap and free (as evidenced by things like books which fortunately for Amazon they foresaw and now sell us everything else instead). It is not just bookshops and libraries who were affected by this seizmic change. Professionals and businesses of all kinds are continuing to see the value of their ‘knowledge’ diminish while their clients knowledge continues to increase and ‘unqualified’ competition stiffen.
The responses to this have been various but in many ways dysfunctional. By focussing even harder on what worked in the past many professionals of all shades have literally driven themselves out of business (look at some taxi firms and Uber for instance).
In Medicine the reaction has been very mixed. Whilst I welcome some recent intiatives to improve patient engagement and make services more patient focussed, these efforts have frequently yielded mediocre results as they are actually glorified customer-focussed data gathering exercises rather than change engines. Such a missed opportunity.
Regulations, Guidelines, Procedures, Repeat
In addition to this in my short 6 years of medicine I have witnessed a stifling increase in regulation to compensate for poor performance. This has largely consisted in the rise of a very rigid system of regulations and checks. This has had the effect of improving the very poor performers at the expense of the best (as in teaching and other public services).
No organisation can really excel if it is constantly trying to meet (sometimes arbitrary) targets. (At this point I must make clear that there are lot of hospitals doing a very good job despite the overwhelming bureaucracy – (I know because I have worked at some of them). However, this doesn’t change the fact that the good is the enemy of the best 1; and you will never get to the best if your efforts are just focussed on meeting targets (WHAT you do?) and improving processes (HOW you do it?). The key is WHY? 2
Why is Why so important?
And this is the problem as I see it: As a country we have lost our healthcare WHY?! The reasons are many but we have become defined by WHAT we do and HOW we do it rather than WHY we do it. If we really cared about WHY we do it then we would do it differently because our still largely acute-illness focussed, pre-internet model of care isn’t working that well anymore for the majority of patients with chronic diseases they have looked up on the internet.
It’s time to stop paying lip service to patient-centered (particularly outpatient) care and start practicing it. You see what we primarily don’t need in my country is a insurance driven model of healthcare, rationing, more doctors (although this would be a nice luxury), more nurses (again would be nice but is not the key) or more fads of management, structure, technology and applications. Instead we need to rediscover our WHY and with it our empathy, compassion, patient-centeredness, team-spiritedness and drive to continually make things better beyond the point where it is about money.
Theirin lies the future of healthcare for anyone who wants to catch the vision. I predict it will be 20 years from now before this really starts to catch on.
If you want to join me in pursuing this? Connect with me on LinkedIn or Follow me on Twitter (I’m a human I prefer connections). If it is not an automessage I will read it. (unless its abusive in which case I won’t.)
In the last couple of weeks I have been contacted by several people who have designed various gadgets for Medical VR/interaction. They are iridescent imaging, VIZR, D-EYE and Gesturetek.
Mitch Downey founded this company to create fantastic small and life-size VR projections.m see more images here: http://iridescentimaging.com The technology looks fantastic but as you might expect it isn’t cheap. I can really see how these might be useful for virtual clinics, particularly in specialties where walking in front of the doctor is a key part of the exam: ie. Rheumatology / Neurology. However, a remarkable product needs a great website and this is something that needs a bit of work.
This thing looks excellent. It can effectively enable an ophthalmologist to diagnose a child remotely in another country using just their smartphone but more likely it will be a great clinic application. To be honest I want one on my emergency unit as it looks so easy to use but again these things are new and therefore costly. https://www.d-eyecare.com
This is more like a clinician assistant (like Google glass) they feel their user interface and information is more up to date. It looks like a smart gadget but as the video on the site demonstrates it is not entirely unobtrusive to the patient looking at the doctor http://www.vizrtech.com
Time will tell whether there will be enough uptake. My feeling is that unfortunately for this device we are still several years away from IoT and the effects of Big Data having their full impact to help this device work.
These guys are doing something a bit different. Trying to get physical controls to work for rehab /those with disabilities. Unfortunately the website is dire which is a shame as they have some really cool products like Irex-an upper and lower extremity training system.
It looks like they are doing a great work in their niche.
Note I have just started a medium blog as well and plan to integrate them later so watch this space.
What surprises me most about the article below is the so far low uptake of Telemedicine. The applications for this are potentially vast but due to various restrictions particularly surrounding the reluctance of US health insurers to fund such consultations, the general uptake is still low.
Several companies in the UK are trying to build these primary care alternatives now (Dr Now, Babylon etc) and it would appear that there is public desire for these things. However, they face lots of challenges.
Firstly patients are offered more comprehensive services in the NHS even if there is a delay to access them; tests are very difficult to organise at home over the Internet; Patients can’t be fully examined and fundamentally there is a major shortage of GPs. This means that capacity is unlikely to ever be able to meet demand in a cost efficient way without adopting alternative models of triage.
These challenges can all be overcome in time but the fundamental test will be what patients actually want. As physicians we think we know the answer to this question but have we really asked the right questions?









 Because the NHS is squeezed from all sides this provides a great escape valve for trusts if the innovation can be scaled and used across the board to improve efficiency. The AHSN’s and other groups have developed to help facilitate this and there are now various financial incentives appearing via NHS reimbursement schemes.
Because the NHS is squeezed from all sides this provides a great escape valve for trusts if the innovation can be scaled and used across the board to improve efficiency. The AHSN’s and other groups have developed to help facilitate this and there are now various financial incentives appearing via NHS reimbursement schemes.













You must be logged in to post a comment.