![]()
There are lots of different kinds of clinical developer but they generally fall into 6 different broad disciplines as represented by the different colours of the octagon above. In a way the disciplines are somewhat artificial, as what really matters is getting results and not which broad category you fall into. For instance you cannot be a frontend developer and not be at least slightly interested in user experience design. However, they help to give others some idea of your background strengths when it comes to building a team.
Note: Not all of these roles even require much coding skill. Some developers can get by without coding at all! I will cover this in future posts.
Clinician Frontend Developer

‘Frontend’ generally pertains to the parts of the website that you as the visitor can see. These developers focus on producing visible web presence. They range from those who rely entirely on pre-built products (this is a completely acceptable way to start and can actually get you quite far as I will show you) to those who code in HTML, CSS, Javascript, SQL and often other languages as well. If your main aim is to produce a tangible web-presence then this is the route you want to take at the start.
Clinician Backend Developer
‘Backend’ is all about the things you can’t see. This type of developer tends to deal with everything from servers and members-only areas on websites, to fully functional web-apps and sometimes whole online platforms. They tend to code in some of the higher-order languages like Python, PHP and Ruby. It is quite difficult to be a backend clinician developer without having at least some basic coding skills. However, there are all sorts of frameworks that make things much easier (I will explain about these as we go on). If you want to build web-algorithms or fully functional websites with members areas etc you will need to know at least some ‘backend’ skills.
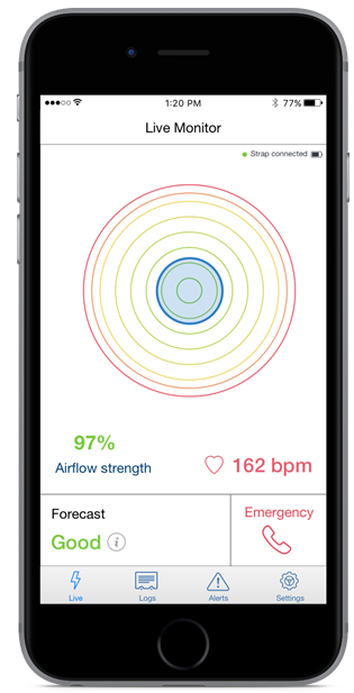
Clinician IoS/Android App Developer
These clinicians focus on phone apps. These require a whole different framework in order to build. I won’t go into it now but this whole area is changing extremely quickly and standalone phone-apps probably aren’t the best way to start-out if you are starting a business. However, once you have an established product there is definitely sometimes a place for building a ‘phone presence’. Some clinicians have built incredibly successful businesses using phone apps.
Clinician Data Scientist

This is my personal area of interest. The clinician data scientist knows how to use computers to solve complex data issues and build algorithms. They generally code in Python or R and use algorithms to analyse data. Machine learning problems are solved by this group and I believe we are only just at the beginning of seeing the impact data scientists will have on our clinical lives. However, the problems specifically require detailed experience and understanding of the problem in order for them to be solved. This is where the clinician data scientist has a massive advantage.
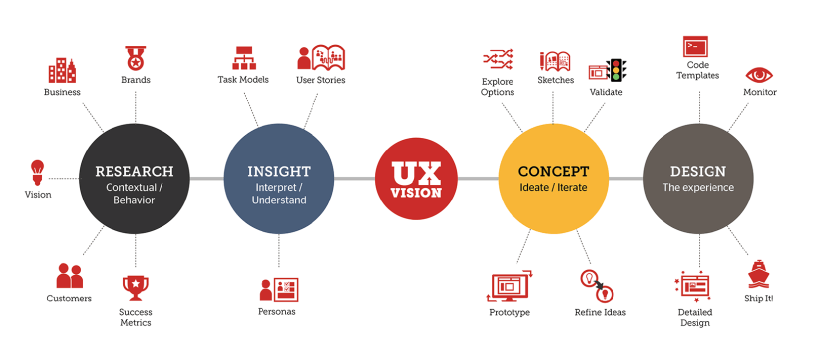
Clinician UX Specialist

UX stands for user-experience design. These clinicians focus on making things flow by reducing ‘friction’ and making things ‘human’ shaped. This can be achieved by relentless testing, market research, attention to detail and most importantly focussing on what would best solve their own problems. The clinician is well placed to be a UX expert as they have deep personal experience of the issues which beset those they care for and fellow clinicians. It requires a very open mindset and is not so much about the technical aspects, although many are very adept coders as well. If anything is going to work it needs good UX to be woven into it.
Clinician Full-Stack Developer

This is the full package. Fluent in many languages they can basically do everything above to a degree but possibly not to the depth of someone well versed in one discipline. If you need one person to test out ideas quickly this person is your best bet. They can also network very effectively with other developers and because they can iterate ‘build’ very quickly they are a real asset to any development team. In the future they will be common but at the moment they are rare.
To find out more visit : www.clinicaldevelopers.org – signup to our mailing list for updates, tips and tricks.


































You must be logged in to post a comment.