Disclaimer: This article is not intended as medical advice for patients but is for informational purposes only, primarily aimed at clinicians.

The liver is supplied by multiple vessels and divided into 8 segments.
In the normal liver most of the blood supply comes from the portal vein.
Tumours however tend to be supplied by the arterial supply (more on this later).
Regarding imaging. Ultrasound is great but unfortunately results are not reproducible between different operators.
 C
C
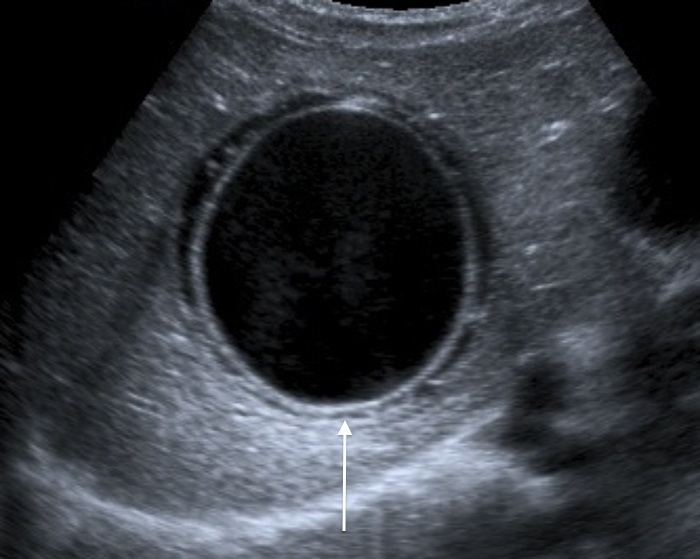
Common benign findings include: Cysts

but sometimes they are not so simple
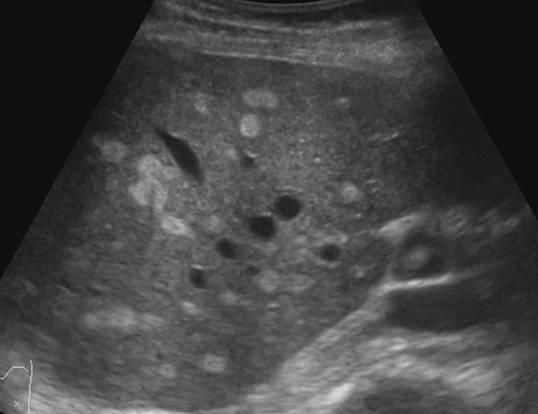
 This one above turned out to be a hyatid cyst (Echinococcosis).
This one above turned out to be a hyatid cyst (Echinococcosis).
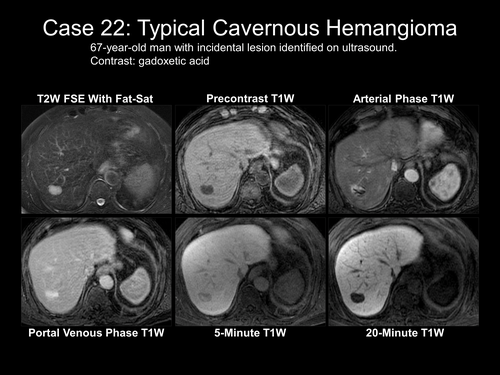
Haemangiomas can be even more difficult to distinguish.
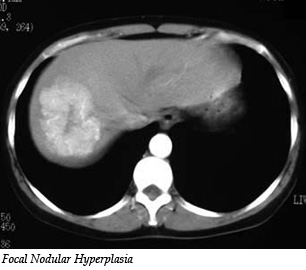
Focal nodular hyperplasia (above) can be distinguished from hepatomas by using Primavist (came out 2004). This contrast is taken up avidly by healthy hepatocytes and not by cancers.
Diffusion weighed MRI can help to distinguish between small metastases and other lesions, however its effectiveness is limited.
Above is a fatty liver which makes it very difficult to distinguish the liver parenchyma

This is what acute hepatitis looks like on USS. The liver looks ‘brighter’.
The radiologist can also see vessels such as varices, abdominal collaterals, reversed/blocked portal flow and associated ascites etc.
Cirrhosis can be seen but only at an advanced stage so these imaging modalities are not so useful for the early detection of liver disease. Of CT, USS and MRI – MRI is the best at picking up cirrhosis but it is also the most expensive and difficult to access test.
Hepatocellular Carcinoma
The above conditions are all benign, but what we really want to spot are the cancers. These primary cancers normally occur in those with pre-existing liver disease.
Diagnosis can be very tricky if the timing goes wrong which is why you need a skilled radiology team.
Above are some images of HCCs. They tend to be surrounded by areas of necrosis as the tumour develops a rim of dead tissue around it.
Treatment options include:
Sorafenib, TACE, transarterial chemoembolization, resection and transplant
This is where we are now in 2016 but there are many other investigation and treatment options under investigation. So we can now tell what’s probably going on without doing a biopsy, most of the time. There is still significant margin for improvement.
Next up: Liver disease in pregnancy.
