Disclaimer: This article is not intended as medical advice for patients and is for general information only.


This is an important but often overlooked area.
A lot of the guidelines on this are over 20 years old.
Malnutrition leads to multiple problems: 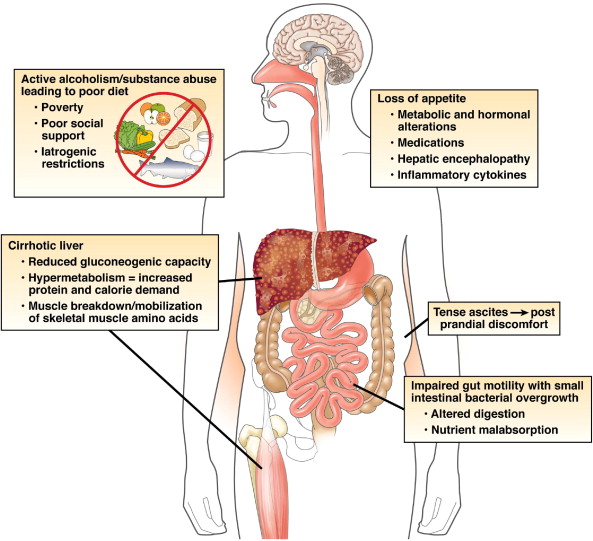
It is a vicious cycle. Particularly with the empty calories of alcohol.
There are often co-existant other medical problems such as: bile salt malabsorption, pancreatic exocrine insufficiency, SBBO, Neomycin.
The goal of treatment is to improve nutritional status and correct micro-nutrient deficiencies. Major options include oral/enteral supplementation or oral nasogastric/jejunal feeding.




All of the above are relatively simple measures to improve nutrition and they can have a dramatic influence on outcomes. In one study 1.Cabre et al patients with acute alcohol related hepatitis were randomised to steroids and nutrition or steroids alone. Only 8% of those who had nutrition plus steroids died, compared to 38% of those who only had steroids (p <0.05). The authors felt that the steroid only group had more infections, explaining the difference in mortality.
Other guidelines by 2. Plauth et al support this conclusion as well as the need for a low salt-diet in liver disease.
References:
- Cabré E, Rodríguez-Iglesias P, Caballería J, Quer JC, Sánchez-Lombraña JL, Parés A, Papo M, Planas R, Gassull MA. Short- and long-term outcome of severe alcohol-induced hepatitis treated with steroids or enteral nutrition: a multicenter randomized trial. Hepatology. 2000;32:36–42.
- Plauth M, Cabré E, Riggio O, Assis-Camilo M, Pirlich M, Kondrup J, Ferenci P, Holm E, Vom Dahl S, Müller MJ, et al. ESPEN Guidelines on Enteral Nutrition: Liver disease. Clin Nutr. 2006;25:285–294.



 C
C
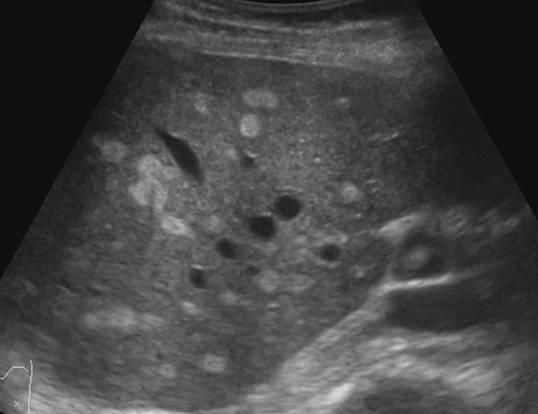
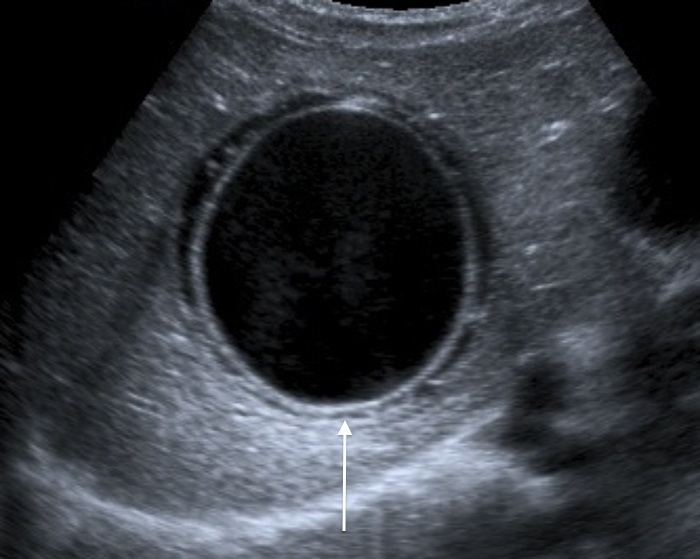 This one above turned out to be a hyatid cyst (Echinococcosis).
This one above turned out to be a hyatid cyst (Echinococcosis).


You must be logged in to post a comment.