Disclaimer: This article is not advice for patients and is intended as information for medical professionals only.
Acute liver failure with encephalopathy (toxic cognitive impairment) has a much worse outcome. Particularly if it comes on insidiously.
This slideshow requires JavaScript.
Acute encephalopathy secondary to paracetamol for instance has a better outcome than that secondary to hepatitis or more chronic causes.
Paracetamol overdose is still by far the biggest cause of acute liver failure in the UK.
Resuscitation, early treatment with N-Acetylcysteine is key and involve ITU early.
Think about hypoglycaemia & hypovoleamia. Crystalloids with glucose and NAC are the mainstay of early management. Give antibiotics if you suspect at risk of infection and call the liver unit early if: history, consciousness, coagulopathy or any other adverse signs.
This slideshow requires JavaScript.
There has been a dramatic improvement in outcomes as a result of the above. Survival is now over 75% of those going to King’s liver unit for acute liver failure.
Transplantation has led to massive improvements in the survival of those with previously a poor prognosis, but the medical management has also improved significantly even for those who cannot be transplanted.
This is in part due to earlier recognition. The average INR of those arriving at King’s has fallen from 6 to 3.5 over the past 15 years and rates of encephalopathy on arrival have improved greatly.
Cerebral oedema is an issue but it is becoming rarer due to early administration of NAC and resuscitation.
Some treatments such as cooling don’t seem to work. Plasma exchange might have a role in the future.
Transplantation particularly has a role in those where the cause is not clear / seronegative disease. Transplantation is not as effective in paracetamol overdose.
Prognostic criteria include: age, coagulopathy and encephalopathy. King’s have produced a new calculator to help distinguish between those who will/won’t benefit from transplant: New King’s Calculator.
Disclaimer: This article is not intended as medical advice for patients and is for general information only.
This is an important but often overlooked area.
A lot of the guidelines on this are over 20 years old.
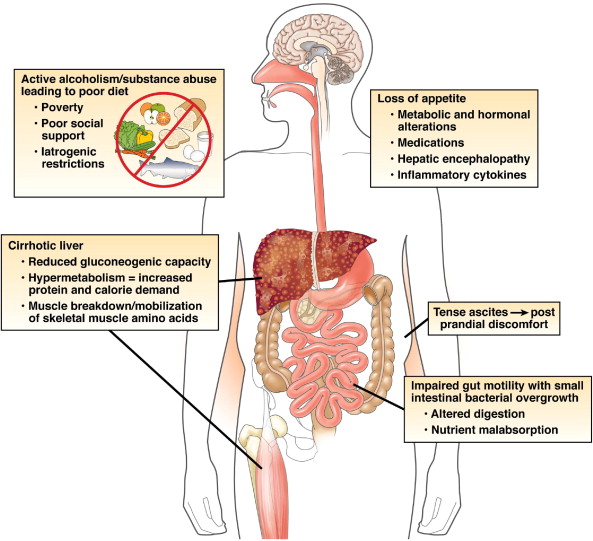
Malnutrition leads to multiple problems:
It is a vicious cycle. Particularly with the empty calories of alcohol.
There are often co-existant other medical problems such as: bile salt malabsorption, pancreatic exocrine insufficiency, SBBO, Neomycin.
This slideshow requires JavaScript.
The goal of treatment is to improve nutritional status and correct micro-nutrient deficiencies. Major options include oral/enteral supplementation or oral nasogastric/jejunal feeding.
PEG tube
Supplement
Supplement
NG/PEG
All of the above are relatively simple measures to improve nutrition and they can have a dramatic influence on outcomes. In one study 1.Cabre et al patients with acute alcohol related hepatitis were randomised to steroids and nutrition or steroids alone. Only 8% of those who had nutrition plus steroids died, compared to 38% of those who only had steroids (p <0.05). The authors felt that the steroid only group had more infections, explaining the difference in mortality.
Other guidelines by 2. Plauth et al support this conclusion as well as the need for a low salt-diet in liver disease.
References:
Cabré E, Rodríguez-Iglesias P, Caballería J, Quer JC, Sánchez-Lombraña JL, Parés A, Papo M, Planas R, Gassull MA. Short- and long-term outcome of severe alcohol-induced hepatitis treated with steroids or enteral nutrition: a multicenter randomized trial. Hepatology. 2000;32:36–42.
Plauth M, Cabré E, Riggio O, Assis-Camilo M, Pirlich M, Kondrup J, Ferenci P, Holm E, Vom Dahl S, Müller MJ, et al. ESPEN Guidelines on Enteral Nutrition: Liver disease. Clin Nutr. 2006;25:285–294.
Disclaimer: This article is not intended as medical advice for patients but is for informational purposes only.
Cirrhosis is when parts of the liver become hardened by damage done over time. Cirrhotic sections of liver unlike normal liver segments cannot repair itself.
Fortunately this is a relatively rare scenario as most patients develop cirrhosis later in life. However, cirrhosis is becoming more common due to rising rates of obesity. Pregnant women with cirrhosis (which may be undiagnosed) can run into difficulty.
The biggest risk is bleeding, because pregnancy leads to an increased circulating volume of blood and the foetus compresses the inferior vena cava.
Most of this bleeding occurs in the oesophagus and normally has to be prevented surgically either by banding of these vessels – called varices or inserting a shunt called a TIPS or transhepatic-portosystemicshunt. Pregnant women should ideally have foetal monitoring while undergoing any procedures.
This slideshow requires JavaScript.
Large liver-specialist centres need to be involved, especially if other problems subsequently develop. Early delivery may sometimes be necessary.
As long as the mother’s health is optimised then the same is normally true for the baby as in normal pregnancy.
Hepatitis
Hepatitis of any kind can be more serious in pregnancy. It needs to be managed with specialist input. Certainly chronic hepatitis B warrants some form of management at some point prior to birth in order to minimise the risk of transmission to the foetus.
Disclaimer: This article is not intended as medical advice for patients but is for informational purposes only, primarily aimed at clinicians.
The liver is supplied by multiple vessels and divided into 8 segments.
In the normal liver most of the blood supply comes from the portal vein.
Tumours however tend to be supplied by the arterial supply (more on this later).
Regarding imaging. Ultrasound is great but unfortunately results are not reproducible between different operators.
C
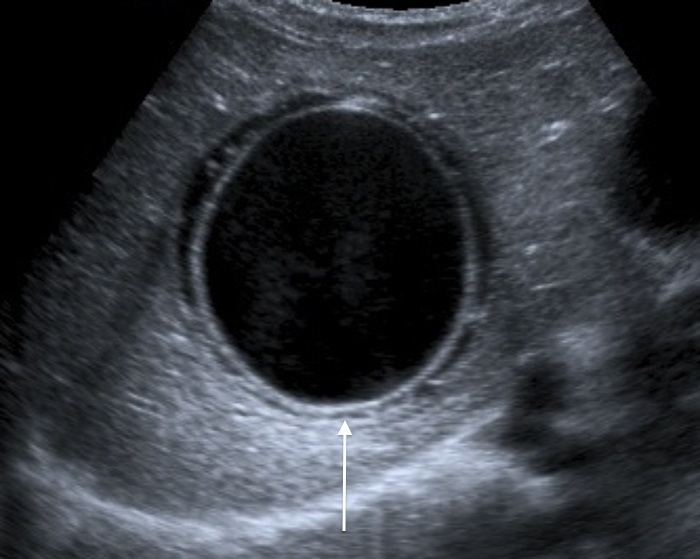
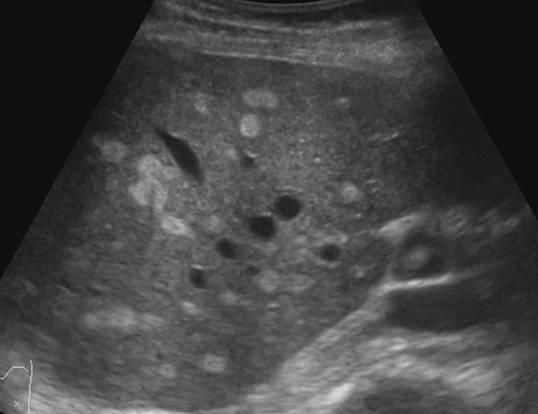
Common benign findings include: Cysts
but sometimes they are not so simple
This one above turned out to be a hyatid cyst (Echinococcosis).
Haemangiomas can be even more difficult to distinguish.
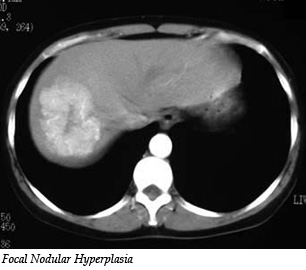
Focal nodular hyperplasia (above) can be distinguished from hepatomas by using Primavist (came out 2004). This contrast is taken up avidly by healthy hepatocytes and not by cancers.
Diffusion weighed MRI can help to distinguish between small metastases and other lesions, however its effectiveness is limited.
Above is a fatty liver which makes it very difficult to distinguish the liver parenchyma
This is what acute hepatitis looks like on USS. The liver looks ‘brighter’.
The radiologist can also see vessels such as varices, abdominal collaterals, reversed/blocked portal flow and associated ascites etc.
Cirrhosis can be seen but only at an advanced stage so these imaging modalities are not so useful for the early detection of liver disease. Of CT, USS and MRI – MRI is the best at picking up cirrhosis but it is also the most expensive and difficult to access test.
Hepatocellular Carcinoma
The above conditions are all benign, but what we really want to spot are the cancers. These primary cancers normally occur in those with pre-existing liver disease.
Diagnosis can be very tricky if the timing goes wrong which is why you need a skilled radiology team.
This slideshow requires JavaScript.
Above are some images of HCCs. They tend to be surrounded by areas of necrosis as the tumour develops a rim of dead tissue around it.
Treatment options include:
This slideshow requires JavaScript.
Sorafenib, TACE, transarterial chemoembolization, resection and transplant
This is where we are now in 2016 but there are many other investigation and treatment options under investigation. So we can now tell what’s probably going on without doing a biopsy, most of the time. There is still significant margin for improvement.
Art meets the microbiome Fantastic art/science fusion blog by this Brighton based artist. We need more of this in medicine and as scientists it helps to keep us grounded in reality.
She has also done a lot of work on microbiological resistance and seeks to raise awareness of this through art. Fantastic!
What happens when clinicians working in the NHS collide with coders and software developers? Awesome stuff is what! That’s the whole point of NHS Hacks – different fields working …
I learned so much from this guy I had to share it with others…
Now is the Time
Why bother starting a lifestyle business. You are sitting on so much value and you want to share that with the world not just make your life easier. you don’t want a checklist business!
‘Big will not beat small anymore. The fast will beat the slow’ — Rupert Murdoch. Even he is aware of it.
Ask yourself: Where can your business be in 12 weeks?
Incumbents should note that there are hidden ‘gun’s’ (startups) in peoples garages which contain bullets with other companies names on them.
As an investor, John Spindler finds the lack of background research by entrepreneurs to be one of the most commonly encountered frustrating problems. To solve this he suggested:
Make 2 columns:
Fact column- 2–3 facts you KNOW about this business plan.
2. Second column- Hypotheses. What things do I need to find out to build this thing?
Work out what is your OPPORTUNITY HYPOTHESIS. Build, Measure, Learn. Call it a project rather than a business because it is easier to fail fast. (I like the psychology of this idea and have already found it helpful).
In the experimental stage check your are measuring the right metrics, evaluation of them will lead to excellent execution.
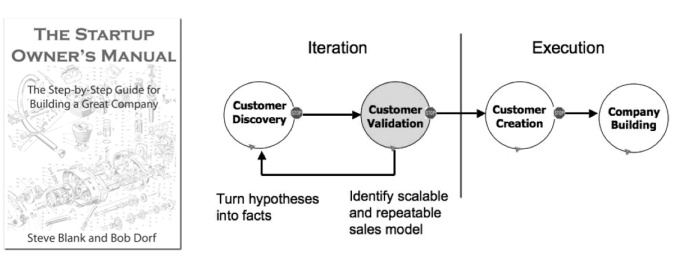
Startup Owners Manual: Steve Blank and Bob Dorf
Don’t build something nobody wants
3 types of advice: validated, negative and useless. (Validated/Negative advice in 8 weeks can be tested to see if it works. Good or bad it will help you. )
However, 95% of advice is useless in the next 8 weeks. Therefore, shelve it because it’s useless to you now.
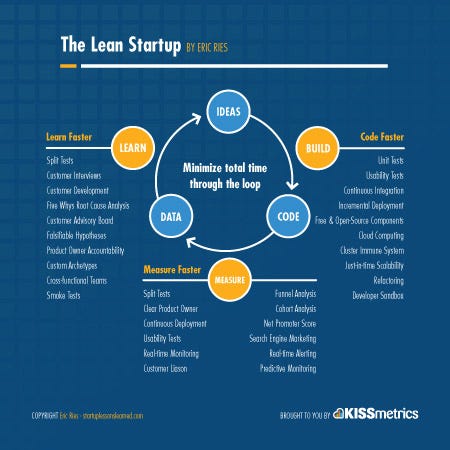
Lean is just about organising the chaos, reducing waste and risk, providing more learning and a common language. IF your core assumption is wrong you need to test that FIRST. Then you will save yourself a lot of time.
It’s a common language. There is jargon and as soon as you learn it you can communicate with others — be ‘in the club’ as it were.
If you are going to build, do a lot of thinking. Then build the thing that teaches you what you need to learn.
The number one thing an investor will look at is the team. If you can convince a quality person to join you that is a sign of success. If you can recruit a quality army this is your number 1 asset! What quality of ARMY can you recruit? Investors will care about this more than anything else as it is the biggest single determinant of success.
Get OTHERS to validate your product. Your own validation is not that valuable but multiple external validations are.
Testing Hypotheses
A good hypothesis is simple & clear, written as a statement, establishes participants (who), variables (what’s involved) and prediction of an outcome (evidence).
The Pepsi Challenge type scenario is NOT the right first validation exercise. You have to assume that the first answer is wrong. Ask 5 why’s & eventually you might get to the nub of it. AVOID CONFIRMATION BIAS like the plague.
Most people are NOT early adopters in ANYTHING. Most people have habits that are very hard to break.
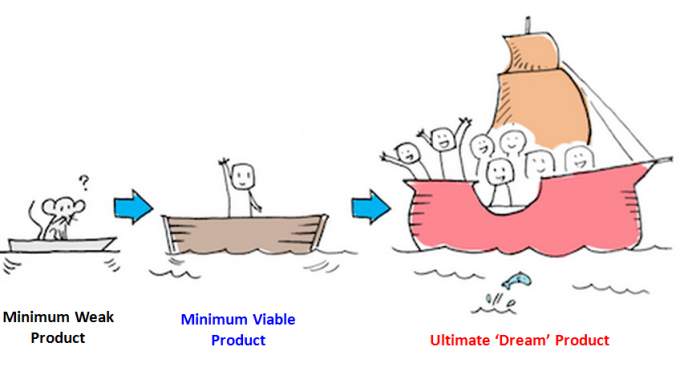
MVP is not a crappy version of the product. It is a prototype. Consierge MVP is legitimate. It can be a simple landing page, it can be a proof of concept, it can be something for people to engage with, it can be a paper prototype, a pitch, fake demo video, or something to help a developer to understand. It is just a way to answer the questions you need to answer.
Consierge means it is not scalable. It’s just there to allow you to learn. Beware, If your hypothesis is circular then its not a hypothesis and you need to think again.
Key assumptions you need to make
At least several other people are working on the same thing right now. How you think this your business idea will work is probably wrong. Your main job is to learn faster than the competitors. That is why the team is the key. It is the process and the people that win NOT the product itself.
The market is not stable and anyone who doesn’t keep moving forward will fall behind.
Call it a project, give it a name, sell something, convince someone else to join, set a goal that will inspire you, live 6 months in the future, fall in love with the problem and not your solution. Follow Peter Thiel’s philosophy as per ‘Zero to One’ (find it on Amazon its a good book.)
Teams
There are two types of teams. Napoleon team — they will follow your every command. The best teams however are people who are smarter than you and can do things you can’t and you bring them on the journey with you. They don’t want to just be footsoldiers for your army.
Bare minimum you need a hipster (domain insight), hacker (builder) and hustler (seller) to succeed.
Paul Graham- You need three things to be a successful entrepreneur — a great team, proof that customers want it and a willingness to do it with minimal money!
Regarding Customers
‘Make something people want’ — Paul Graham, Y Combinator
Avoid wasting too much time trying to change the ‘stuck’ middle who don’t want to innovate because they are very good at using the current system. Are your people your assets or your problem?
Before building your business ask: What problem would someone else solve for me?
Another thought: The number of secrets in the world is roughly equivalent to the number of startups we need.
How did the companies that are currently successful scale. When you scale big you win even if your product is inferior. Unless you can bring 10* value you are unlikely to be able to displace an incumbent. (As per Peter Thiel).
Design Thinking
He would thoroughly recommend doing Stanford’s online course on design thinking (8–10 hours). Emphasise, define, ideate, prototype, test. Do it in groups if you can, it will radically transform your thinking.
‘Kick Ass’ products have evidence that they solve a customers problem in a big market. Focus on the early adopters. People you can beta test with. Commit 5 people. They need to know they are aren’t buying a perfect solution.
They are trying to find a home made solution. They want you to succeed, they will give you their time and honest feedback and you have a relationship of trust. Your mum is not one of these first customers!
Do you know the demographic? Needs and goals? Problems that need solving, Present behaviours? How do they go about solving those problems? Reference group? The behaviours and the psychology are key.
Behaviour Change
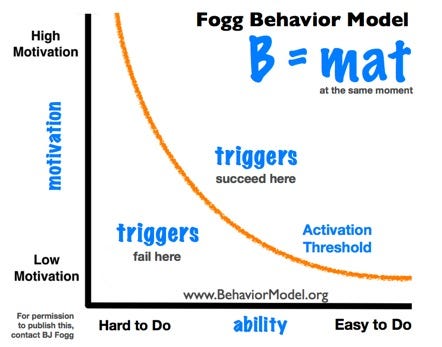
BJ Fogg. Head of behavioural theory at Stanford. B=mat. B=behaviours, m=motivation, a=pre-acquired ability, t=triggers (we are all contextual. We need external triggers to get us to change our behaviour. Every product is a behaviour change. Activation threshold affected by these three things, the triggers have to be enough to get them over the threshold.
Source: B.Fogg (Stanford) Site as per diagram.
Can you make something better than it already is? make something simpler? In an ideal world how would this problem be solved? Better, Simpler or emerging methods?
He suggests we build 5 actual profiles of 5 potential customers (actual people) . The more specific the better: Motivation, Habit , Income, Age, Location, Status, Backstory. Become intimately acquainted with there problems.
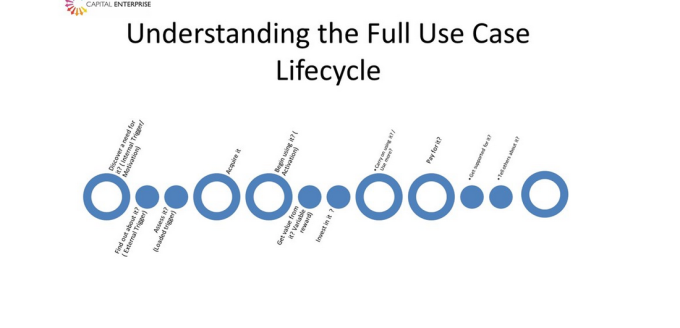
Then understand the full use-case lifecycle.
Source: @capenterprise — John Spindler
What do these personas do when ‘triggered?’
Entrepreneurship is a career. Startups are risky experiments. You don’t have to experiment full time. Start today with what you have.
Do you invest in startups who don’t use lean methodology? Yes but its rarer. Sometimes people just get damn lucky and hit a home run of first base but its the exception rather than the rule and it might not be repeatable.
Then he talked about financing and how ‘founders fit’ and how investors look at these things. Do you have someone resourceful, someone who can do x and y. The team you build now might well not be the team that takes it to the next level. Identify the task in hand and see if the team members can get you there.
Funders and investors must fit. An investor should never distort the function of the startup because this is your task. You have the hands on the controls. They are investing in you!
Suggested reading: Moms test by Rob Fitzpatrick, Running Lean by Ash Maurya and Lean Startup by Eric Ries.
This article came out of notes I took on a talk by @capenterprise at the first NHS clinical entrepreneurs pit stop – The beginning of a new journey. Or see my medium blog
Good legal governance leads to credibility. Helps us to maximise value and avoid costly disputes.
£130,000 to get to court
£600,000 to take a case through the IP court!
Good examples of Patents that have succeeded: Ermil who developed the can pull and then sold it to coca cola.Before long he was making a lot of money with his few cents take per can!
Is your idea actually YOURS? If it is can you obtain freedome to operate and therefore commercialise the idea. In order to do thsi it will need to be protected.
Learning from Lord of the Rings. Keep it secret. Keep it safe. Or more correctly keep it confidential, keep it safe.
As soon as you start to disclose the core of your stuff you need a NDA in place. As good practice you should still be trying to minimise the information you are giving (the secret sauce as it were). When you come to contracting make sure that there are things in place to stop people getting the full picture (drip feed the information).
Patents:
Consider if it is needed, can you afford it, can you afford to defend it, is it patentable.
If you do need one write it yourself because someone else won’t know your idea as well as you!
To Incorporate or not?
Sole trader, partnership or PLC? What to choose. There are advantages and disadvantages to each. If you do incorporate you have protection but you have to decide:
How you divide up the shares in the company.
Creator, founder, entrepreneur, manager, funder. Look at the contributions now and future contributions and then decide how to divide up the stakes. You are looking to make up an equity split.
Documents, articles, officers, directors etc. Lots of things to think about.
What is the rule book – governance of the corporate structure.
Shareholders agreements whill cover all of this. What are the rules. Who are the directors and who are the shareholders. governance, IP, how to transfer shares, dispute resolution, restrictions and leaver provisions are all in here.There needs to be a structure to protect the shares.
Its about building a contractual mechanism to resolve these disputes in order to avoid a court case later on.
Employees
Must have contracts but can have policies which fit everyone.
Your employess represent an operational risk. HR can be tough!
Confidentialitiy, IP ownership, Restrictions and Policies, One size fits all.
Our IP
National contracts do not talk about IP however, local policies might say that individuals do not own IP if they are working in the context of their trust.
Tony suggested potentially writing to the employer explaining that you are building something in your own time and that it is your own IP but also being willing to work with the NHS to make things better for patients.
Roger explained that it is a negotiation.
The whole room is massively engaged at this point
As a businessperson you should also sign up to an LPA just in case something happens to one of the founders. Make wills which tie in your shares, Assignment of intellectual property and other agreements.
Business Model and Contracts
SAP (standard operating procedures) and quality control – document this so you can demonstrate ‘due process’. Also trading contracts whether they be NDA’s, standard terms, bespoke contracts. Don’t sign it if you don’t understand it. and contracts
Bespoke contracts. key terms, compliance, reflect – make sure it fits with your business model and insurance cover. Negotiate.
Joint ventures are particularly important to get right. Define contributions, milestones, outputs. Licences – Get the scope and the outputs correct.
A contract should be a ‘living document’- it needs to keep up to date with the business!
Financing Options
Venture capitlists – are they scary? The key is to find the right VC. If they don’t fit don’t work with them.
Because the NHS is squeezed from all sides this provides a great escape valve for trusts if the innovation can be scaled and used across the board to improve efficiency. The AHSN’s and other groups have developed to help facilitate this and there are now various financial incentives appearing via NHS reimbursement schemes.
The Clinical entrepreneur programme has come about precisely because this need has been recognised. Late definitely beats never, and this in conjunction with the NHS accelerators will hopefully start to gain traction and lead to #development.









 C
C
 This one above turned out to be a hyatid cyst (Echinococcosis).
This one above turned out to be a hyatid cyst (Echinococcosis).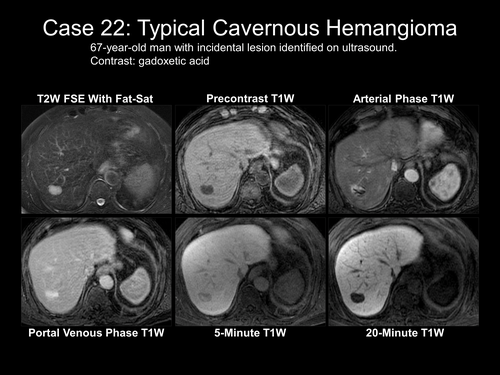






 Because the NHS is squeezed from all sides this provides a great escape valve for trusts if the innovation can be scaled and used across the board to improve efficiency. The AHSN’s and other groups have developed to help facilitate this and there are now various financial incentives appearing via NHS reimbursement schemes.
Because the NHS is squeezed from all sides this provides a great escape valve for trusts if the innovation can be scaled and used across the board to improve efficiency. The AHSN’s and other groups have developed to help facilitate this and there are now various financial incentives appearing via NHS reimbursement schemes.
You must be logged in to post a comment.